Sample Seminar Report Certificate Format 1hn3y
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 445h4w
Overview 1s532p
& View Sample Seminar Report Certificate Format as PDF for free.
More details 6h715l
- Words: 82
- Pages: 1
YOUR COLLEGE NAME
DEPARTMENT OF INFORMATION TECHNOLOGY
CERTIFICATE This is to certify that the seminar entitled “Augmented Reality” is submitted by MYNAME bearing Reg No. ********* in partial fulfillment of the requirement for the award of the degree Bachelor of Technology in Information Technology of YOUR COLLEGE NAME for the academic year 2017-2018.
Miss. Lecturer Seminar Coordinator Assistant Professor Information Technology Place: Placename Date: 12/12/2017
Mr. Lecturer Mrs. Lecturer Seminar In charge Head of the Department Senior Lecturer Information Technology Information Technology
DEPARTMENT OF INFORMATION TECHNOLOGY
CERTIFICATE This is to certify that the seminar entitled “Augmented Reality” is submitted by MYNAME bearing Reg No. ********* in partial fulfillment of the requirement for the award of the degree Bachelor of Technology in Information Technology of YOUR COLLEGE NAME for the academic year 2017-2018.
Miss. Lecturer Seminar Coordinator Assistant Professor Information Technology Place: Placename Date: 12/12/2017
Mr. Lecturer Mrs. Lecturer Seminar In charge Head of the Department Senior Lecturer Information Technology Information Technology
Related Documents 2w1qw
Sample Seminar Report Certificate Format 1hn3y
November 2021 0
Sample Seminar Report Acknowledgment Format 2w476j
October 2019 3,616
Sample Seminar Report Front Page Format 610f
November 2021 0
Format For Seminar Report 2m1m52
December 2019 133
Seminar Report Format 3gh47
December 2019 134
B.tech Seminar Report Format 2a5s4p
December 2019 202More Documents from "Afsal" 5s3u5u
Sample Seminar Report Certificate Format 1hn3y
November 2021 0
Sample Seminar Report Acknowledgment Format 2w476j
October 2019 3,616
Sample Seminar Report Front Page Format 610f
November 2021 0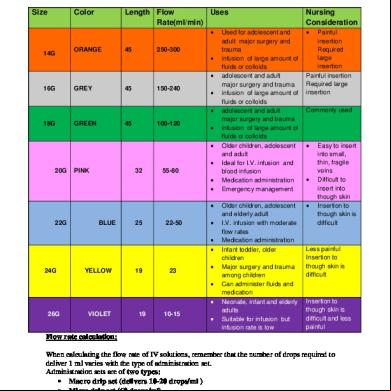
Sizes Of Iv Cannulas And Flow Rate Calculations p74c
October 2019 114
The 4v6835
October 2019 144